Diabetic Retinopathy
If you have diabetes, your body does not use and store sugar properly. High blood sugar levels can damage blood vessels in the retina, the nerve layer at the back of the eye that senses light and helps to send images to the brain. The damage to retinal vessels is referred to as diabetic retinopathy.
Diabetic retinopathy, the most common diabetic eye disease, occurs when blood vessels in the retina change. Sometimes these vessels swell and leak fluid or even close off completely. In other cases, abnormal new blood vessels grow on the surface of the retina.
Diabetic retinopathy usually affects both eyes. People who have diabetic retinopathy often don’t notice changes in their vision in the disease’s early stages. But as it progresses, diabetic retinopathy usually causes vision loss that in many cases cannot be reversed.
There are two types of diabetic retinopathy:
Nonproliferative diabetic retinopathy (NPDR)
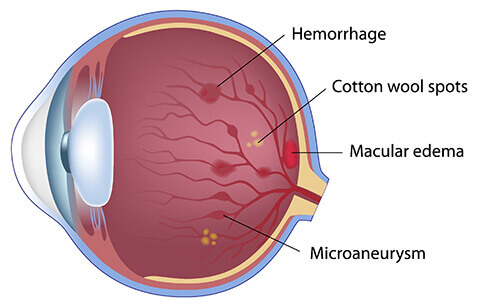
NPDR is the earliest stage of diabetic retinopathy. In this stage, tiny blood vessels within the retina leak blood or fluid. The leaking fluid causes the retina to swell or to form deposits called exudates.
Many people with diabetes have mild NPDR, which usually does not affect their vision. When vision is affected it is the result of macular edema and/or macular ischemia.
Macular edema is swelling or thickening of the macula, a small area in the center of the retina that allows us to see fine details clearly. The swelling is caused by fluid leaking from retinal blood vessels. It is the most common cause of visual loss in diabetes. Vision loss may be mild to severe, but even in the worst cases, peripheral vision continues to function.
Macular ischemia occurs when small blood vessels (capillaries) close. Vision blurs because the macula no longer receives enough blood supply to work properly.
Proliferative diabetic retinopathy (PDR)
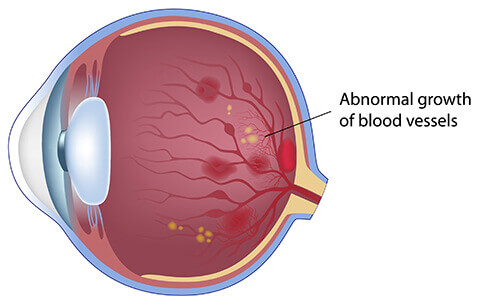
Proliferative diabetic retinopathy (PDR) mainly occurs when many of the blood vessels in the retina close, preventing enough blood flow. In an attempt to supply blood to the area where the original vessels closed, the retina responds by growing new blood vessels. This is called neovascularization. However, these new blood vessels are abnormal and do not supply the retina with proper blood flow. The new vessels are also often accompanied by scar tissue that may cause the retina to wrinkle or detach.
PDR may cause more severe vision loss than NPDR because it can affect both central and peripheral vision. PDR affects vision in the following ways:
- Vitreous hemorrhage: delicate new blood vessels bleed into the vitreous — the gel in the center of the eye — preventing light rays from reaching the retina. If the vitreous hemorrhage is small, you may see a few new, dark floaters. A very large hemorrhage might block out all vision, allowing you to perceive only light and dark. Vitreous hemorrhage alone does not cause permanent vision loss. When the blood clears, your vision may return to its former level unless the macula has been damaged.
- Traction retinal detachment: scar tissue from neovascularization shrinks, causing the retina to wrinkle and pull from its normal position. Macular wrinkling can distort your vision. More severe vision loss can occur if the macula or large areas of the retina are detached.
- Neovascular glaucoma: if a number of retinal vessels are closed, neovascularization can occur in the iris (the colored part of the eye). In this condition, the new blood vessels may block the normal flow of fluid out of the eye. Pressure builds up in the eye, a particularly severe condition that causes damage to the optic nerve.
What are the symptoms of diabetic retinopathy?
You can have diabetic retinopathy and not be aware of it, since the early stages of diabetic retinopathy often don’t have symptoms. As the disease progresses, diabetic retinopathy symptoms may include:
- Spots, dots or cobweb-like dark strings floating in your vision (called floaters);
- Blurred vision;
- Vision that changes periodically from blurry to clear;
- Blank or dark areas in your field of vision;
- Poor night vision;
- Colors appear washed out or different;
- Vision loss.
- Diabetic retinopathy symptoms usually affect both eyes.

How is diabetic retinopathy treated?
The best treatment is to prevent the development of retinopathy as much as possible. Strict control of your blood sugar will significantly reduce the long-term risk of vision loss from diabetic retinopathy. If high blood pressure and kidney problems are present, they need to be treated.
- Medical Treatment: In certain cases, CNY Eye physician may choose to treat your macular edema with injections of medicine in your eye. These special shots of medicine—called intravitreal injections—may be steroids or other medications. They are designed to shrink the swelling of the macula or reduce neovascularization.
- Laser surgery: Laser surgery is often recommended for people with macular edema, PDR, and neovascular glaucoma. For macular edema, the laser is focused on the damaged retina near the macula to decrease the fluid leakage.
- The main goal of treatment is to prevent further loss of vision. It is uncommon for people who have blurred vision from macular edema to recover normal vision, although some may experience partial improvement. A few people may see the laser spots near the center of their vision following treatment. The spots usually fade with time but may not disappear.
- For PDR, the laser is focused on all parts of the retina except the macula. This panretinal photocoagulation treatment causes abnormal new vessels to shrink and often prevents them from growing in the future. It also decreases the chance that vitreous bleeding or retinal distortion will occur. Multiple laser treatments over time are sometimes necessary. Laser surgery does not cure diabetic retinopathy and does not always prevent further loss of vision.
- Vitrectomy: In advanced PDR, your ophthalmologist may recommend a surgery called a vitrectomy. During this microsurgical procedure, which is performed in the operating room, the blood-filled vitreous is removed and replaced with a clear solution. Your ophthalmologist may wait for several months to see if the blood clears on its own before recommending a vitrectomy. If the retina is detached, it can be repaired during the vitrectomy surgery. Surgery should usually be done early because macular distortion or traction retinal detachment will cause permanent visual loss. The longer the macula is distorted or out of place, the more serious the vision loss will be. Vision loss is largely preventable.
- Diabetes: If you have diabetes, it is important to know that today, with improved methods of diagnosis and treatment, a smaller percentage of people who develop retinopathy have serious vision problems. Early detection of diabetic retinopathy is the best protection against loss of vision. You can significantly lower your risk of vision loss by maintaining strict control of your blood sugar and visiting your ophthalmologist regularly.
When should I schedule an examination?
People with diabetes should schedule examinations with CNY Eye Physicians & Surgeons at least once a year. More frequent medical eye examinations may be necessary after a diagnosis of diabetic retinopathy. Pregnant women with diabetes should schedule an appointment in the first trimester, because retinopathy can progress quickly during pregnancy. If you need to be examined for eyeglasses it is important that your blood sugar be consistently under control for several days when you see your ophthalmologist. Eyeglasses that work well when blood sugar is out of control will not work well when blood sugar is stable. Rapid changes in blood sugar can cause fluctuating vision in both eyes even if retinopathy is not present.
You should have your eyes checked promptly if you have visual changes that: affect either one or both eyes; last more than a few days; are not associated with a change in blood sugar. When you are first diagnosed with diabetes, you should have your eyes checked: within five years of the diagnosis if you 29 years old or younger; within a few months of the diagnosis if are 30 years old and older.